It astounds me that I have not seen this chart once in the New Zealand media (or from any of our political and bureuacratic officeholders – I hesitate to call them “leaders”).
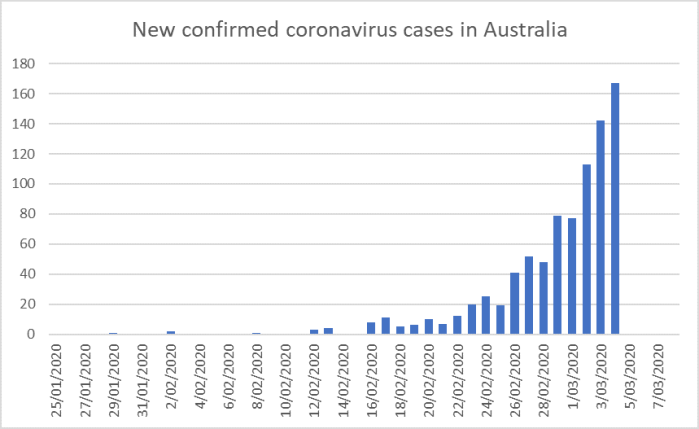
Australia confirmed their first “community outbreak” case on 3 March, when there were 33 cases in total (just fewer than we had yesterday).
It is much the same locally-exponential pattern we’ve seen in so many other countries. If current rates of increase continue then by the end of tomorrow Australia will have per capita numbers akin to those in the US or UK yesterday. That is the sort of impact exponential growth has.
There was routinely a lot of trans-Tasman travel. There is, apparently, still a lot of travel this way as people try to get home. And while in the last few days self-isolation was supposed to be practiced, there are numerous stories of it simply not being following consistently. My worst one was a story someone told me the other day: they’d gone to the hairdresser, who was young and pregnant. The hairdresser passed on the story of a customer who’d come in the previous day and commented that while she was in self-isolation she really needed to get her hair done. The hairdresser, perhaps unsurprisingly burst into tears.
All this means that one can think of New Zealand and Australia as having been essentially a Common Virus Area – what is mine is yours, and what is yours is mine. Since we haven’t been doing the sort of aggressive mass testing that some have called for – although the pace has stepped up in the last few days – it seems simply irresponsible for the government to be running policy on the presumption that we do not have community out break here. No one can be certain, but the question has to be what is the safer assumption to make decisions on right now. Given the rest of the world, given Australia, given the lags (when you confirm community outbreak you should wish you’d acted a couple of weeks earlier), the only sensible approach now is to assume presence, and act accordingly. But apparently in an interview on Newshub this morning, the government’s chief official on health matters said they were still assuming the opposite, staking a great deal on their view being right.
I see the Prime Minister is to speak at midday. We’ll see what she says.
For me, I’m less interested in specific announcements or new rules, but on whether there is evidence that (a) they are going to break with the past and actually take the public into their confidence and engage on the issues, options, costs and risks, (b) whether they finally are willing to front with the public on the severity of what is to come, health or economics, (c) whether there is any sign of a developed stable framework for thinking about policy responses through time (d) whether they any sense of an exit strategy for whatever approaches they adopt, (e) whether there is any sign they have identified what things they belief to be more important than public health in this specific situation, and (f) whether they have thought through seriously how sustainable, economically or socially, whatever strategy they adopt is, or whether they are still just attempting to buy “a bit more time” and risking lurching again before long.
These are difficult issues, and few leaders here or abroad seem to be handling them at all well, but no one made any of them take office.
I had been planning to write a post today prompted by the economic and other policy choices and trade-offs implied by the very useful Imperial College paper published earlier in the week, but I might now come back to that – and particularly questions about whether suppression strategies are worth the costs to the economy and society and its freedoms and values, if anything like what the Imperial College authors suggest it implies were to be an accurate representation of the issue.
UPDATE: Unfortunately, the PM’s statement did not seriously or adequately address any of the sorts of issues raised in the paragraph a couple above.

What about this chart We are not ahead of it
Bad testing, 2 wks late
LikeLike
Precisely. The Ministry is persisting with its rationing of testing – only permitting it on persons who meet the “case definition”, which means limited to persons themselves recently abroad or having had contact with someone recently abroad. This means that even if a GP suspects Covid-19 infection, they will have a request for the test denied by a laboratory gatekeeper unless there is a foreign connection. Perfect way to avoid recognising community spread until some GP is brave enough to lie on a request form.
The other thing about testing is that the test (at any rate when done on nasal or throat swabs, is not very sensitive. That is, there are going to be false negatives, probably in upwards of 20 to 30% of cases and even more of asymptomatic persons incubating the disease. This doesn’t seem to be being realised by people who really should know better. The GP interviewed on breakfast TV on Friday morning stated that he had been self islolating because of contact with a colleague who had been exposed, but had come out of isolation when the colleague’s test came back negative. Not very rational. If the self isolation had been justified to begin with, the negative test was not sufficient grounds on which to stop.
LikeLike
The world never counted Covid19 until China locked down it’s cities. The level of global community spread suggests the timeline is wrong. More than likely this disease has just been treated as the ordinary flu for more than a year already with the USA recording 30,000 deaths as due to the ordinary flu last year.
LikeLike
Getgreatstuff, did you copy this direct from the PRC propaganda machine?
LikeLike
Not really CCP propaganda. It is just simple maths.
LikeLike
Seems to be too much focus on stopping people doing things relative to working on fixing things.
This situation is equivalent to war. The Govt should be marshalling the best professional, academic and business brains and resources to identify issues and work on solutions. Doesn’t seem much evidence of that in the media at least.
LikeLike
A more relevant chart is how many people have died speaking as a person in a very vulnerable age groups. Here in OZ we still have hot temperatures which should reduce the spread of the virus as opposed to the northern Hemisphere. It could well get worse as the temperature drops.
LikeLike
Yes, both fair points. although even without many deaths the hospital resource required even for severe non-fatal cases appears to be considerable.
LikeLike
Unfortunately you are correct.
LikeLike
Hi Michael,
If you plan to write a response to the IC paper it is worth reading Shen, Taleb, and Bar-yam’s review.
https://necsi.edu/review-of-ferguson-et-al-impact-of-non-pharmaceutical-interventions
LikeLiked by 2 people
Thanks. I wasn’t so much thinking of a response – not my expertise – but more about the economic and societal implications of their modelling results, as modified by various points others have made. But I will read the review with interest.
LikeLike
That chart will be us soon
Sent from BlueMail
LikeLike
Browsing around and listening to the chatter over the past 48 hours
The various actions taken by governments and central bankers so far imply a (hoped for) short duration to the problems
When Bernanke set the ball rolling with TARP in 2008 there was an underlying expectation the crisis would pass within 6 months and everything would return to normal
Now, all the authorities are acting on the basis the virus pandemic will pass within the next 6 months
Closing schools and borders and paying businesses to maintain employment is a short term solution – 6 months – after that requires a different mindset. The world-wide tourism industry will not recover for at least one year if not longer. Hotels, Motels, Restaurants (in NZ) are laying off staff and appear not to be retaining their workforce in keeping with the government’s support program
I am no cheer-leader of Rod Oram at newsroom, but the subtext of his article today articulates the hoped-for short-termism of the actions
https://www.newsroom.co.nz/pro/2020/03/21/1091099/unprecendented-havoc-unorthodox-remedies
LikeLike
Even some experts think it will be around a while.
https://www.nzherald.co.nz/business/news/article.cfm?c_id=3&objectid=12316929&&ref=topbox
LikeLike
Just read the Taleb et. al. Article posted above. Well worth the 5 minutes.
LikeLiked by 1 person
South Australia (or at least the large state-owned pathology lab) added covid-19 to its standard respiratory virus panel 3 weeks ago. That needs to happen in NZ now. It’s do-able clearly.
Other news here: the cruise ship that returned from NZ this week with 4 covid-19 cases on board does not seem to have hit headlines in NZ – either the infection was picked up in NZ or the passengers may have spread it in ports (or both). Unless they didn’t dock in NZ??
Nearly every covid-19 story is a tale of too little too late. A shocking failure of public health advice that might have been excusable in January but is bordering on criminally negligent in late March.
LikeLike
Yes, that cruise ship was apparently in Wgtn last Saturday.
LikeLike
I’m interested in knowing the false negative and false positive rates for the Covid-19 tests. I’ve read about a person who was tested twice and came up negative both times, only to develop the virus. he self isolation policies for travellers should take care of most of the false negatives, but it’s human nature to relax when you think no-one’s looking or you’re not actually a risk
LikeLike
Establishing the sensitivity and specificity of any diagnostic test is fraught, mainly because there is seldom a reliable reference standard (persons you know for sure have or don’t have the condition). Another problem is that the test characteristics are not constant – they change with the stage and severity of the disease (incubation, early, late, convalescent), where the specimen is taken (seems to be very much of an issue for SARS-Cov-2), how the specimen is transported, and the technical details of things like RNA extraction and the primer sequences used in the PCR).
Very little yet in the medical literature, but one paper from China shows that PCR on swabs taken from the nose and throat had rather poor sensitivity. (Wang, Xu et al. 2020). Since these are the specimens most likely to be taken in general practices, it is a matter for concern.
Wang W, Xu Y, Gao R, Lu R, Han K, Wu G, Tan W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA. 2020 Mar 11.
LikeLike
Further to my previous reply. There will be a way to work out sensitivity and specificity of tne Covid-19 PCR testing when serology tests can be appled to look back at patients on whom the PCR has been done (serology tests look at antibodies to the virus in serum. Since antibodies take time to appear, these tests are necessarily retrospective). Serological tests for Covid-19 are at present only available at a few reference centres such as Westmead in Sydney.
LikeLike
Depends on the test: sputum 72% sensitivity and nasal swab has 63% sensitivity, whereas the more invasive bronchi-alveolar lavage is 93%. Such estimates are preliminary – from a paper in JAMA by Wang et al. (Open Access)
LikeLike
This seems a more up-to-date chart
https://www.health.gov.au/news/health-alerts/novel-coronavirus-2019-ncov-health-alert/coronavirus-covid-19-current-situation-and-case-numbers
New cases relatively stable at ~110ish/day for the last 4 days. So more of a linear than exponential increase?
Also interesting is the age distribution, centered on the 30-39 and 40-49 cohorts
LikeLike
Thanks. The total numbers as at the end of yesterday are the same 874 or 5 in both sources. I have been using https://en.wikipedia.org/wiki/2020_coronavirus_pandemic_in_Australia. A friend who is doing intensive statistical analysis on the outbreaks across the world (and passing it to NZ govt agencies) is pretty confident the situation in Aus is explosive, at least absent immediate v aggressive interventions.
LikeLike
As a (massive) aside, a non market shock requiring non market responses: should financial markets remain open? The current demand for liquidity given the uncertainty could spiral uncontrollably; but then again, shuttering before opening in calmer times would likely provide material gains for those that were ‘in’ at the point of closure…??
LikeLike
Hard to know. The benchmark extreme case was at the start of WW1 and the intense financial crisis then. the US – not even in the war – closed the stock exchange for 3 months.
I’m always wary of closures and short-selling bans etc, but if someone could make a fairly iron-clad case re the damage from leaving them open, I could be persuaded. But any serious hint of closing would only exacerbate the panic just prior to the action, esp as we have no clear horizon at which the uncertainty and underlying volatility might settle.
LikeLike
Hello Michael
I am also amazed at the tone of the NZ government response to this, as it seems that the balance of risks would favour a much stronger and immediate response. The “upside” of adopting a low level response relative to a “lock down” when the overseas experience suggests rapid community spread (in the absence of a lockdown) are low; and the downside is enormous. Whatever happened to the adage “ A stitch in time saves nine”?
In Morocco, where I am currently living, the government was also a slow but the horror occurring in our three most important neighbours (Spain, France, Italy) led to a very rapid response. Morocco has about 4 million citizens living and working in these countries. Our infected numbers are very similar to those in NZ (under 100, but climbing quickly, relative to a population of 35 million), and the reported numbers are probably an underestimate by a large number. The first case was March 2; there were 12 by March 13 when a cabinet minister caught it overseas. On March 13 the borders with Algeria, Spain and France were closed; (Italy had stopped travel to Morocco earlier); by March 15 all travel overseas was stopped and has remained closed since. Schools and Universities were shut down on March 13, and where I am teaching we were running online courses after 2 days. Restaurants, cafes, gyms, etc were shut down on the 15th/16th; also mosques. Yesterday at 6pm there was full lock-down preventing public gatherings and travel (except local shopping for essential supplies – not sure how this works ) and only people with official authorisations are allowed to travel or be in public spaces. Morocco has a large number of police who are always in the community and it is almost certain that the restrictions will be closely monitored and obeyed. The army has been converting its medical facilities for public use. There is an economic package aimed at ensuring workers in affected industries (particularly hospitality and tourism) obtain some income, and a charity fund started by the government to help those in need ( I don’t know how this works either.) A large number of salaried people, particularly those in state owned businesses, are donating a month’s salary
.
Morocco is a constitutional monarchy with a history of very centralised power and the current King (Mohammed VI) is traditional (head of the Islamic faith) modernising (particularly with respect to female rights) and educated (PhD from France). It is possible that the early infection of a cabinet minister shocked the government. Who knows? However, once the penny dropped the cabinet is not going to look back and ask “Did we respond too slowly?”
I suspect things are worse here than we know, simply because the city centres are very crowded. Fez is famous for its packed medina, where 100,000 people live in a tiny tightly packed maze of alleys and streets (so tightly packed there is no car access for much of the centre). You don’t want to think about this. But I am willing to bet there is no-one wandering around, and the country might be like this for a while.
I can only hope that Morocco’s response works – I suspect it will be another country you will hear more about soon, given its proximity to Europe and the nature of its response. Next time you hear “hard and fast”, here is an example.
Best wishes
Andrew
LikeLiked by 1 person
Thanks Andrew. That is sufficiently striking I’ve linked to your comment on Twitter. What is really striking in NZ is the proportion of the gen public not really taking it seriously at all: some sort of magic thinking that somehow NZ is uniquely exempt.
LikeLike
As a member of the public, I have been rather sceptical that this is a new Chinese virus. Given the level of community spread and the increased numbers due to more tests, I am suspicious that this is actually a new disease and the timeline for the spread is just woefully wrong.
The USA has had a really bad season of the so called ordinary flu with 30,000 deaths to date and worldwide for than 300k to 400k. As the US and the rest of world have never previously tested for covid19, it is highly probable that it is a US virus with the timeline starting a year or more ago.
LikeLike
Full corrected data worldwide
https://covid.ourworldindata.org/data/ecdc/full_data.csv
Australia:
Total cases 920, last daily +172 (at 21/3) (last day not in the csv file yet)
https://www.worldometers.info/coronavirus/country/australia/
Fitting a polynominal to the observed data (from cases=1) gives circa 1600 cases within 3 days (i.e. +74 within 3 days from 920)
New Zealand 52 cases as of 21/3 (last day not in the csv file yet)
Fitting a polynominal to the observed data (from cases=1) gives circa 120 cases within 3 days (i.e. double within 3 days)
NZ needs to go into lockdown.
LikeLike
Thanks. As of now Aus showing 1065 cases, so well on the way.
LikeLike
BBC – The Real Story – Coronavirus: The economic crisis
Just how bad will the downturn be and can anything be done to soften the blow
https://www.bbc.co.uk/programmes/w3csydff
A world view by 4 world economists
53 minute podcast
LikeLike
We are just about to see the economic effects in NZ. Hobbiton 241 redundancies, Queenstown will be in the 2,000 plus (from a reliable source), Air NZ 3,000+, hotels 1,000s??, restaurants etc, who knows? South Island ski fields are thinking they wont even open as the costs are too high.
Migrant fruit and grape pickers have apparently returned home, I have already seen a Kiwifruit company appealing for pickers and packers for the same reason.
LikeLike
Fruit picking?
https://www.rnz.co.nz/news/national/412305/otago-farmers-nervous-about-labour-shortage-from-border-restrictions
LikeLike
The lobbyists are getting in for their chop
$57m to be spent on Māori coronavirus response package
Includes
– $10 million for whanau Māori community outreach
– $15 million to Whānau Ora to reach into Māori communities
https://www.stuff.co.nz/national/health/coronavirus/120473692/57m-to-be-spent-on-mori-coronavirus-response-package
And
Tourism Industry Association Chief Executive Chris Roberts said tourism businesses across the country had “no customers, no revenue, and no choice”. He warned mass lay-offs would soon become necessary if a UK-style bailout package wasn’t considered.
And
Jim Boult mayor of Queenstown (and former Director and Deputy Chairman of Tourism NZ) got a sit-down with PM at the Beehive day-after the $12.1 bn package announcement
LikeLike
I’ve watched the tourism industry for 30 years (as a bus driver).
Real wages have tracked downwards.
Markets collapsed (Japan) but others appeared (Taiwan). The Japanese married NZrs and some stayed (with residency) During that period they had paid top rate for coach hire.
Meanwhile
Chinese drivers appeared, gradually outnumbering NZrs. Every other street has a house with a Mercedes Sprinter up the drive or Mitsubishi Rosa (and trailer) on the street (hey will all be on income support).
The local newspaper, Mountain Scene was full of this property developer and that property developer.
Bus yards squeezed for space.
According to Bloomberg and Financial Times NZ is “overtourismed”
LikeLike
https://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=12318501
Article indicates 2.5% of cases need ICU.
NZ has 176 beds at the moment so roughly we cant have more than 7,040 active infections at any one twim without overloading the system (this assumes the ICUs are all in the right places)
Article discusses 300 ICUs in another model which give 12,000 active cases.
Given the difficulty of moving patients between ICUs in different parts of the country the max cases we might be able to cope with could be 80%, or 5,632 & 9,600 respectively.
We need either massive suppression to keep the case load down or more ICUs.
LikeLike
https://www.theguardian.com/commentisfree/2020/mar/21/the-case-for-shutting-down-almost-everything-and-restarting-when-coronavirus-is-gone
Have to admit I’m a fan for:
Endgame C: stop then restart
Endgame C is to “stop then restart”. This means minimising activity and interactions, and sealing the borders to passenger traffic including citizens (although not trade), until infections are driven down to zero.
The economic damage from an ongoing pandemic for 12-18 months until there is a vaccine with cases sitting at ICU capacity has to be far more costly that curfewing everyone for 8 – 12 weeks.
LikeLike
Going out on a limb and extrapolating NZ’s data from cases=1, & 66 cases as of today, with a polynominal we will be at circa 5,500 cases in a month (this is our ICU capacity at 176 ICU beds at 2.5% needing ICU from above)
https://ourworldindata.org/coronavirus-source-data
LikeLike
Turkey promotes quick diagnostic kits for coronavirus
Reliability of kits very high, says expert
https://www.aa.com.tr/en/latest-on-coronavirus-outbreak/turkey-promotes-quick-diagnostic-kits-for-coronavirus/1774589
Useful if true.
LikeLiked by 1 person
Hi Michael
This is a very gois article about the lack if evidence-based policies…
https://www.statnews.com/2020/03/17/a-fiasco-in-the-making-as-the-coronavirus-pandemic-takes-hold-we-are-making-decisions-without-reliable-data/
If you look up research on Google scholar Re for example school closure during pandemic you might wonder if the gov decision is right?
LikeLike